ABSTRACT
Aim Vascular pathologies have been already explored for the most of their aspects. It is a group of pathologies with unclear ethology and with an evolution in time not easy to forecast. Treatment guidelines are conflicting. The aim of this study was to describe cases in their most practical and technical aspect, especially in complicated conditions.
Methods This was a descriptive case report of a patient with a hepatic artery aneurysm complicated by a dissection leading up to the splenic artery, and how the team had invented a planned treatment for the patient using a minimally invasive approach. The experience was born with the intention of showing how the endovascular approach is at least as safe as the traditional one despite the complexity of our case.
Results The procedure was completed without any complications. After a stay in long day surgery, the patient returned home. Conclusion Using a minimally invasive technique allows to reduce the patient’s post-operative suffering and the economic burden on the health system.
INTRODUCTION
Visceral artery aneurysm (VAA) is an uncommon form of vascular pathology (1). Patients with VAAs present various symptoms up to symptomaticity with acute rupture and abdominal pain, and haemorrhagic shock (1,2). Thanks to the increased usage of imaging such as ultrasound, CT and MRI, nowadays it is also possible to individuate VAAs as occasional reports (1,3). The VAAs have multiple aetiologies. They can be caused by trauma (2), inflammatory or infectious conditions (2), and some iatrogenic post-surgical causes are also reported (2). In particular, an increased incidence of splenic artery aneurisms has been described in pregnant women, because of an increased blood flow to the spleen (4). Macroscopically, VAAs can be associated with splenomegaly, multiple pregnancies, portal hypertension, pancreatitis, coronary artery disease, peptic ulcer or gastritis, obesity. The male to female ratio is 1:2 (4). Unlike the other VAAs, hepatic artery aneurism occurs most commonly in males rather than females, probably because of the differences in the pathogenesis of this form (4). Moreover, the prevalence of hepatic artery aneurism has increased due to the increase in the number of diagnostic and therapeutic procedures in the biliary tract (5). The vessels most frequently involved are: splenic (60%), hepatic (20%), superior mesenteric (5%) and celiac (4%) arteries; rarely gastroduodenal, renal, pancreatic duodeal, jejunal, ileocolic and inferior mesenteric arteries (1). In association with the dilatation of the vessel, there are some typical pathophysiological alterations: fybrodysplasia, intimal thickening, sclerosis, hypercholesterolemia (2). In case of rupture, the mortality rate is between 21% and 100% (from hepatic artery aneurysm rupture to celiac one) (1). Because of the VAAs discovering at autopsy, it is necessary to have a more aggressive diagnostic and treatment approaches (1), and patients with a high risk of rupture such as pregnant or symptomatic, should be treated (3). The aim of this study was to report endovascular surgical procedure of a patient presenting an aneurysm of the hepatic artery complicated by a dissection of the splenic artery.
PATIENT AND METHODS
Patient and study design
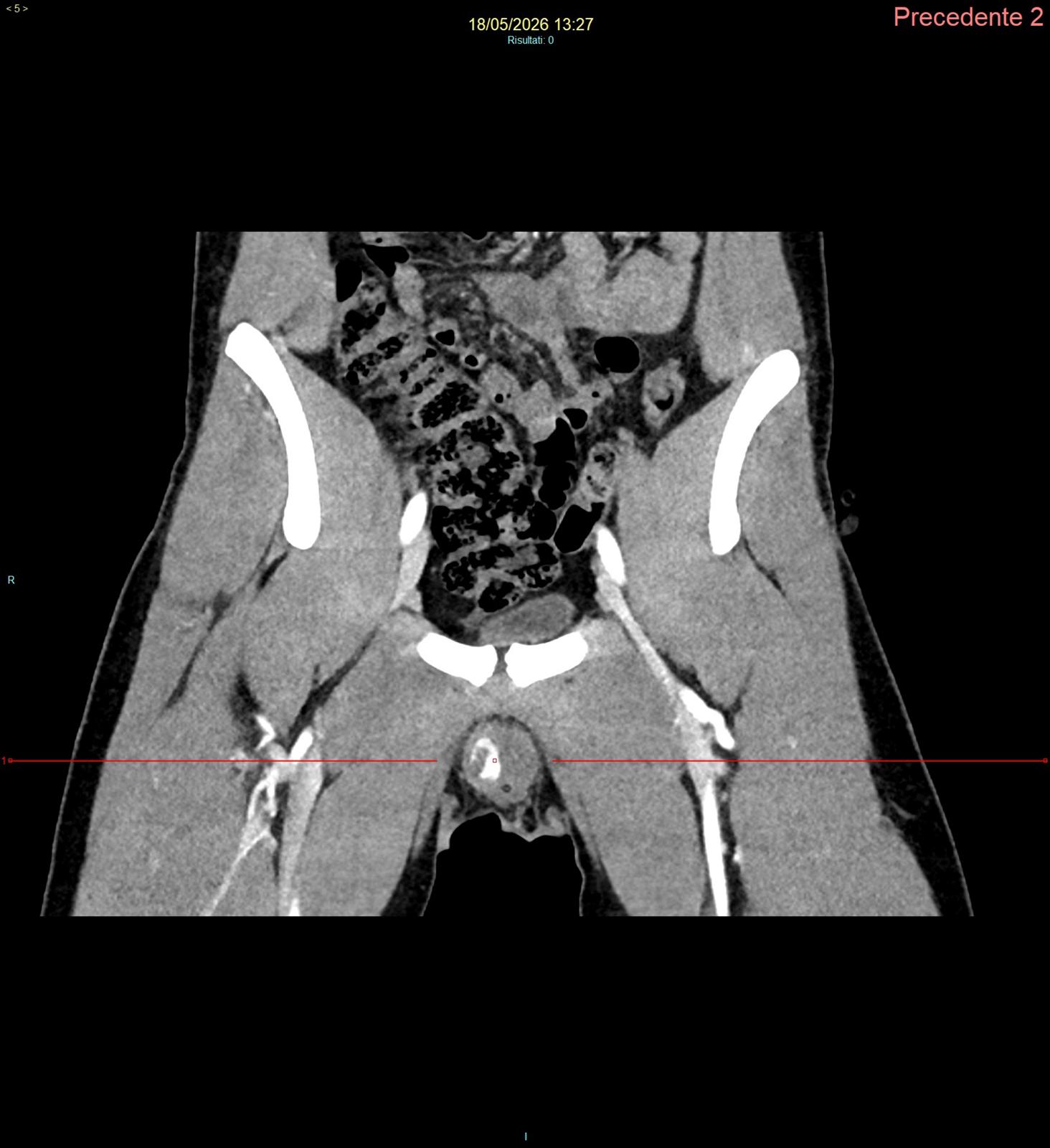
A 56-years patient, male, arrived to our observation at the Emergency Department of the P.O. Ospedale del Mare, Naples, during November 2019 for a violent nocturnal abdominal angina. Laboratory test revealed Hb 12g/dL, normal values of AST/ALT, bilirubin 1.3mg/dL. Abdominal CT with contrast showed the presence of a celiac trunk dissection and an aneurysmal dilation of the hepatic artery, greater than 2cm; therefore, he was amenable to surgical treatment (Class IIa, level C, Società Italiana di Chirurgia Vascolare ed Endovascolare – SICVE guidelines) (7) even though complicated by the splenic artery originated from the false lumen of the celiac trunk (Figure 1).
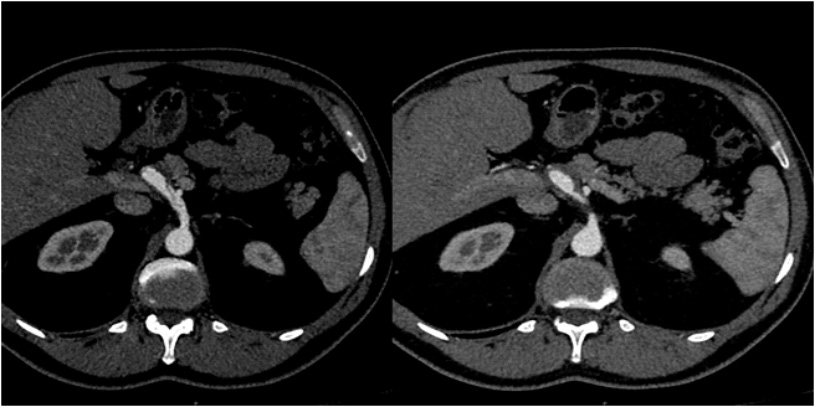
Figure 1. Angio-computed tomography (CT) cross sections show celiac trunk dissection (left); celiac trunk aneurysmal sac (right) (P.O. Ospedale del Mare, ASL NA1 Centro, 2019)
After a consultation with vascular surgeons, it was decided to perform a tailored endovascular treatment for this patient. The patient was informed in a clear and comprehensive way of three types of treatments and other possible surgical and conservative alternatives. A surgical consent confirmed that clinical data can be used for scientific studies but remain anonymous.
Methods
The “Santini” technique – description. Through the same arterial access, two guides were inserted and then landed separately in hepatic and splenic arteries. Local anaesthesia (10 mL carbocaine 2%) was practiced in the groin before the femoral puncture. An introducer (8F, Cook, Flexor, Germany) was positioned through the right femoral artery. Then, a selective arteriography of the celiac trunk was executed and it showed a dissection at the origin 145 of the trunk and the presence of a double lumen: a true one and a false one. From the false one, the splenic artery originated and the true one fed the aneurysmal sac of the hepatic artery (Figure 2).
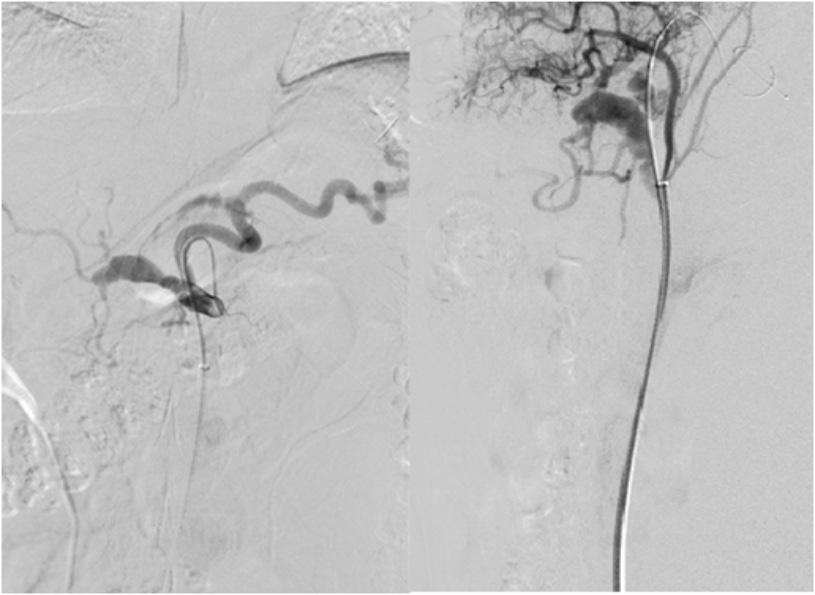
Figure 2. Pre-treatment digital subtraction angiography (DSA) angiographic control: contrast opacification of celiac trunk, splenic artery and hepatic artery aneurysm (left); lateral view of the contrast opacification of the aneurysm sac and a guide positioned in the splenic artery (right) (P.O. Ospedale del Mare, ASL NA1 Centro, 2019)
The false lumen and the splenic artery were catheterized and Supracore guide was introduced with the distal end at the splenic hilum (Figure 3A); the aneurysmal sac was catheterized by micro-catheter (Progreat Terumo, USA) (Figure 3B). The aneurysmal sac was then embolized with controlled realising spirals (Interlock, BS) and free spirals (Vortex, BS, USA) until a total filling and exclusion from the circle (Figure 4A). Afterwards, a self-expanding covered stent (8×60 mm, Covera, Bard, USA) was hooked to the origin of the celiac trunk until the origin of the splenic artery (Figure 4B).
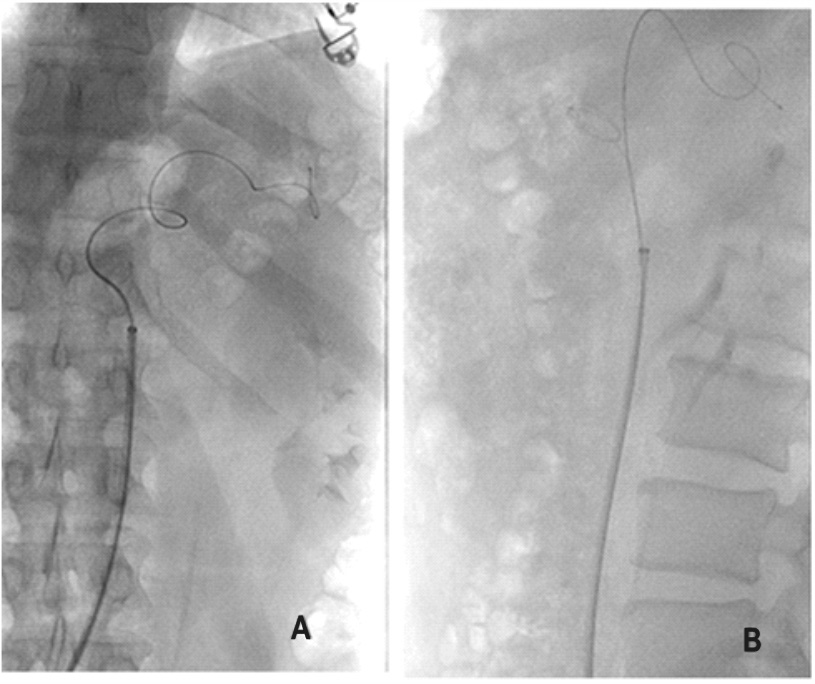
Figure 3. A) Supracore guide at the splenic hilum; B) aneurysm micro-catheterization with Progreat Terumo (P.O. Ospedale del Mare, ASL NA1 Centro, 2019)
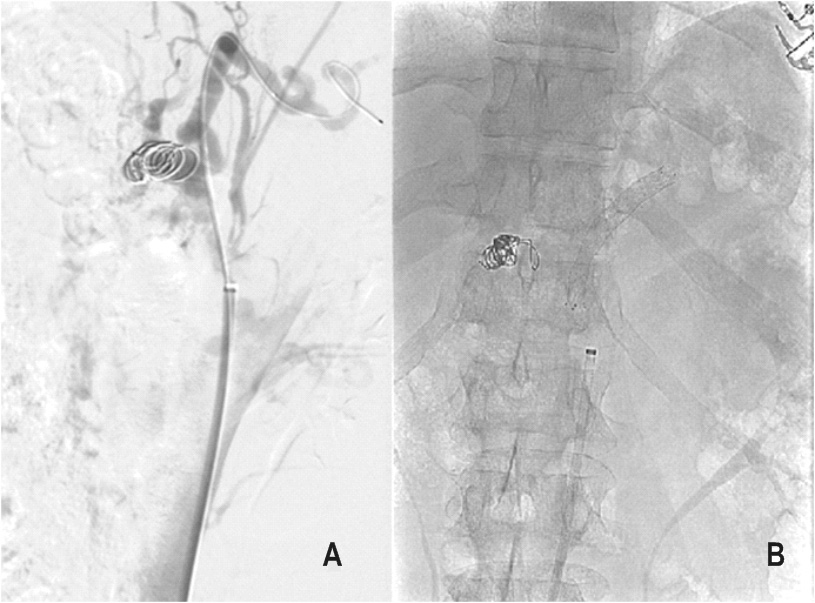
Figure 4. A) Aneurysmal sac embolization with controlled releasing spirals; B) self-expanding covered stent positioning (P.O. Ospedale del Mare, ASL NA1 Centro, 2019)
RESULTS
Procedural angiographic control showed total exclusion from the circle of the aneurysmal sac and the patency of the splenic artery (Figure 5). The procedural angiographic control showed an opacification of the splenic artery that contained the covered stent, the celiac tripod and the total exclusion of the aneurysmal sac that appeared embolized by the spirals (Figure 5). Then a manual compression manoeuvre was performed and a compression bandage applied in the inguinal right area; after 24h under observation, the patient was discharged, scheduling an angiographic CT control at one month. The subsequent check-up showed the perfect success of the operation, which was intended precisely not to allow the traumatic lesions to expand (Figure 5). Furthermore, by landing the covered stent before the birth of the left gastric artery, it was saved (Figures 5).
DISCUSSION
The VAA is a rare but potentially life-threatening disease entity. Early diagnosis and treatment are critical for the prevention of rupture. In the past years the increased use of ultrasound, CT and MRI and improved definition of the image have allowed the discovery of many cases of asymptomatic aneurysms (1). Despite a definitive diagnostic gold standard is not univocal, CT–angiography is highly accurate in the diagnosis and helps in determining the most correct approach, thanks to multiplanar CT reconstructions (8). An indication for the treatment should derive from existing symptoms, or in cases of asymptomatic patients it can be determined based on the risk of rupture that corresponds with the diameter of the aneurysm (5).
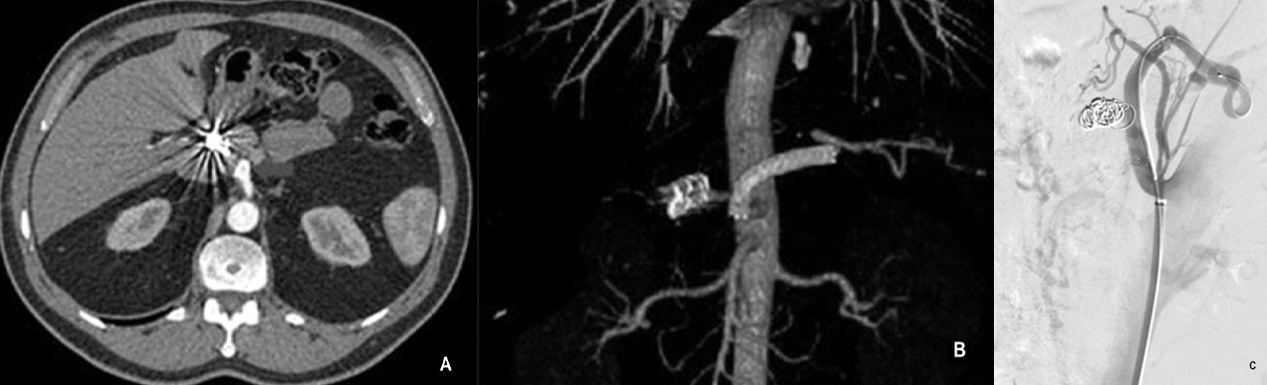
Figure 5. A) Post treatment angio-computed tomography (CT): the white arrow indicates the presence of the covered stent from celiac trunk to splenic artery; B) 3-D reconstruction of the post procedural angio-CT; C) Post treatment angiography shows the stent positioning and the spirals presence (P.O. Ospedale del Mare, ASL NA1 Centro, 2019)
In the patient described above it was necessary to intervene with this new technique due to the presence of a double pathology: dissection and aneurysm on the celiac trunk with the splenic artery originating from the false lumen. Some studies state that an aggressive open surgical approach is justified despite the VAAs could be asymptomatic, because of low morbidity and mortality, and the endovascular approach has to be reserved for some cases not better specified (6). Due to considerable surgical trauma associated with a conventional open procedure and a surgical mortality rate that is not to be underestimated, the endovascular treatment of visceral artery aneurysms has significantly gained the importance (1). The indications for the elective treatment of visceral artery aneurysm are made from a diameter of 2 cm (5). In case of isolated visceral artery dissection in a hemodynamically stable patient, medical therapy is primarily considered; in case of unstable lesions, the surgical approach is preferred (6). This approach is supported by many authors who demonstrated that hemodynamically unstable dissections gradually increase in length and tend to involve other visceral arterial vessels with a significant increase of mortality, with phenomena of liver thrombosis, rupture of arterial vessels, therefore, the intervention is strongly suggested (5). In literature, due to the rarity of this pathology, there is a lack of studies comparing the outcome between open or endovascular technique, although the interventional radiologic approach is increasingly chosen (3), not only as an emergency choice in the first instance, but also with, as in this case, a tailored treatment and programmed technique. The endovascular treatment of visceral aneurysm is already the treatment of choice in polytraumatized patients (6). In our case, an interventional radiological approach was chosen in accordance with recent guidelines (7). From the technical approach point of view, during the setting, first the hepatic artery was embolized through spirals. This approach was possible for two main reasons that consented to preserve hepatic vascularization: the hepatic parenchyma is supplied for 70% by the venous system and therefore it should not suffer of the lack of arterial supply, and we also performed a meticulous rescue of the left gastric artery allowing the liver to be supplied by the gastro-duodenal circulation. The “Santini” technique was born “from the need” to resolve the dissection of celiac-splenic relevance with the exclusion of the aneurysm. Although the goal of our intervention was firstly not focused on the treatment of splenic artery dissection, the treatment of tripod aneurysm allowed the resolution of both lesions. All of the visceral aneurysms (VAAs) are an uncommon type of pathology, but to find a hepatic artery aneurysm complicated by a dissection of the splenic artery, let us say it, is pretty rare. The purpose of our case, as of all the literature about rare events, was initially to collect and show cases for kicking a stream of sharing. Secondly, to propose a new and never seen approach in treating vascular pathologies using the mini-invasive approach and all of its advantages, thanks to the endovascular surgery. Stetting graph offers a potential benefit of maintaining splenic perfusion while excluding the aneurysm, thereby eliminating the risk of rupture (5). Moreover, because of the high mortality risk in case of rupture of VAAs and dissections, the treatment by embolization or stenting is preferable as the first choice. Naturally, the support of vascular surgeons remains essential in case of complications, even during the endovascular procedure.
Gianpaolo Santini1, Pasquale Quassone2, Luca Tarotto1, Francesco Arienzo1, Giuseppe Sarti1
1Vascular and Interventional Unit-P.O. Ospedale del Mare, ASL NA1 Centro, viale delle Metamorfosi, 2Department of Precision Medicine, University of Campania “L. Vanvitelli”; Naples, Italy
REFERENCES
1. Laganà D, Carrafiello G, Mangini M, Dionigi G,Caronno R, Castelli P, Fugazzola C. Multimodal approach to endovascular treatment of visceral artery aneurysms and pseudoaneurysms. Eur J Radiol 2006; 59:104-11. 2. Abbas M, Stone W, Fowl R, Gloviczki P, Oldenburg W, Pairolero P, Hallett J, Bowe T, Panneton J, Cherry K. Splenic artery aneurysms: two decades experience at Mayo Clinic. Ann Vasc Surg 2002; 16:442-9. 3. Tulsyan N, Kashyap V, Greenberg R, Sarac T, Clair D, Pierce G, Ouriel K. The endovascular management of visceral artery aneurysms and pseudoaneurysms. J Vasc Surg 2007; 45:276-83. 4. Panayiotopulps Y, Taylor P, Assadourian R. Aneurysm of the visceral and renal arteries. Ann R Coll Surg Engl 1996, 78:412-9. 5. Pitton M, Dappa E, Jungmann F, Kloeckner R, Schotten S, Wirth G, Mittler J, Lang H, Mildenberger P, Kreitner K, Oberholzer K, Dueber C. Visceral artery aneurysms: Incidence, management, and outcome analysis in a tertiary care center over one decade. Eur Radiol 2015; 25:2004-14. 6. Chiesa R, Astore D, Guzzo D, Frigerio S, Tshomba Y, Castellano R, Liberato de Moura MR, Melissano G. Visceral artery aneurisms. Ann Vasc Surg 2005; 19:42-8. 7. Stillo F, Ebner H, Lanza G, Agus GB, Apperti M, Bernardini E, Bianchini G, Camparini S, Crespi A, De Fiores A, Dorigo W, Emanuelli G, Ferrara F, Genovese G, Giacomelli E, Giannasio B, Gossetti B, Musiani A, Quarto G, Sellitti A, Spinelli GM. Linee guida sicve-sif societá italiana di chirurgia vascolare ed endovascolare e societá italiana di flebologia [The 2016 Guidelines of the Italian Society for Vascular and Endovascular Surgery (SICVE) and Italian Society of Phlebology (SIF)] [In Italian] Italian Journal of Vascular and Endovascular Surgery 2016; 23:1-45. 8. Sun G, Ding J, Lu Y, Li M, Li L, Li G, Zhang X. Comparison of standard and low tube voltage 320 detector row volume CT angiography in detection of intracranial aneurysms with digital subtraction angiography as gold standard. Acad Radiol 2012; 19:281-8.